
Arthroscopic subacromial decompression and acromioplasty is a minimally invasive keyhole procedure to treat shoulder bursitis, bone spurs and impingement symptoms. It is often done as a part of other keyhole procedures in the shoulder, such as a biceps tenodesis and rotator cuff repair. After an isolated arthroscopic subacromial decompression and acromioplasty a sling is worn for 1-2 weeks; and JPL therapy commences immediately after surgery. Strengthening is allowed at 4-6 weeks; and full unrestricted activity is possible at 6-12 weeks after surgery. This pathway may vary if other procedures are carried out at the same time.
This is a surgical procedure that is performed keyhole (arthroscopic) to remove the inflamed bursa and bone spur below the acromion. This is usually done as a day procedure or with an overnight stay, depending on what else is being addressed within the shoulder.
The keyhole procedure has some advantages compared to more traditional open methods of surgery (with larger incisions), they include:
The essential components that are treated during a subacromial decompression and acromioplasty are:
The other possible areas that may be simultaneously treated (either diagnosed on MRI prior to surgery or found at the time of arthroscopy):
The procedure is performed under a General Anaesthetic where you will be positioned on your side and the affected arm secured in a special arm holder.
Biceps
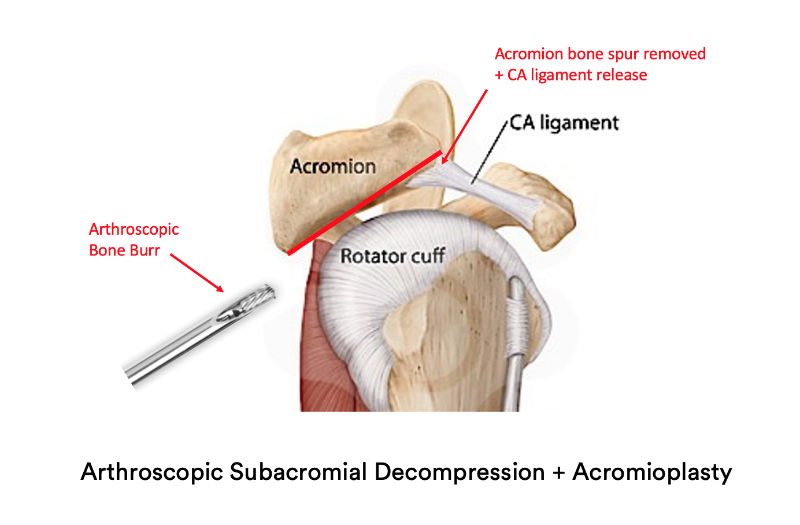
Bone Spur and Bursa
Dr Pant will then organise close follow up at regular intervals and liaise with your Physiotherapist to maximise your recovery.
The outcome after a subacromial decompression and acromioplasty is generally excellent with surgical wounds barely visible ultimately. Patients commence therapy immediately after surgery using the JPL protocol. They can dispense with the sling after the first week or two and commence driving after the wound review appointment (at 2 weeks). The only exception to this is if a Rotator Cuff Repair or Biceps tenodesis has been carried out – in which case a sling is worn for six weeks and driving commences at 6-8 weeks.
There are three essential components to a good outcome from surgery
Post-operative physiotherapy
Dr Pant utilises the JPL pathway for most patients and this will form the basis of your rehabilitation after surgery; it will be modified to suit your individual circumstance.
The JPL pathway allows for self-directed, early passive shoulder range of movement:
Therapy overview
After the surgery you will be in a sling and protect your shoulder to allow the shoulder to heal. At two weeks after the surgery Dr Pant will see you at your review appointment and discuss the JPL rehabilitation protocol with you. This JPL physiotherapy protocol will commence two weeks after your surgery.
The therapy program will focus on flexibility and range of motion exercises initially. These gentle stretches will improve your range of motion and prevent shoulder stiffness. As the shoulder begins to heal you will be able to progress to exercises that strengthen your shoulder muscles. Shoulder strengthening is commenced at 4-6 weeks post isolated subacromial decompression and acromioplasty surgery.
Sling
The type of sling is selected specific to you and your shoulder surgery
Driving after shoulder surgery
Showering and getting dressed
Sleeping after Shoulder Surgery
Elbow and hand movement
Surgery is a carefully choreographed process and you are being treated by a sub-specialist shoulder surgeon and a highly experienced team; however, all surgeries inherently carry some risk of complications.
The risk of complications after arthroscopic subacromial decompression and acromioplasty surgery are less than 1% in the Sydney Shoulder Unit experience. General risks include:
Specific risks relating to arthroscopic subacromial decompression and acromioplasty surgery:
Patients who smoke, use tobacco products, have diabetes, or are elderly are at higher risk of complications both during and after surgery. They are also more likely to have problems with wound and bone healing.
Most healthy patients, however, cope well with keyhole shoulder surgery and are unlikely to have complications.

Dr Sushil Pant is a leading Australian trained orthopaedic shoulder surgeon. He is the founder and medical director of the Sydney Shoulder Unit; and is a Shoulder Surgeon at Sydney Sports Medicine Centre at Sydney Olympic Park.
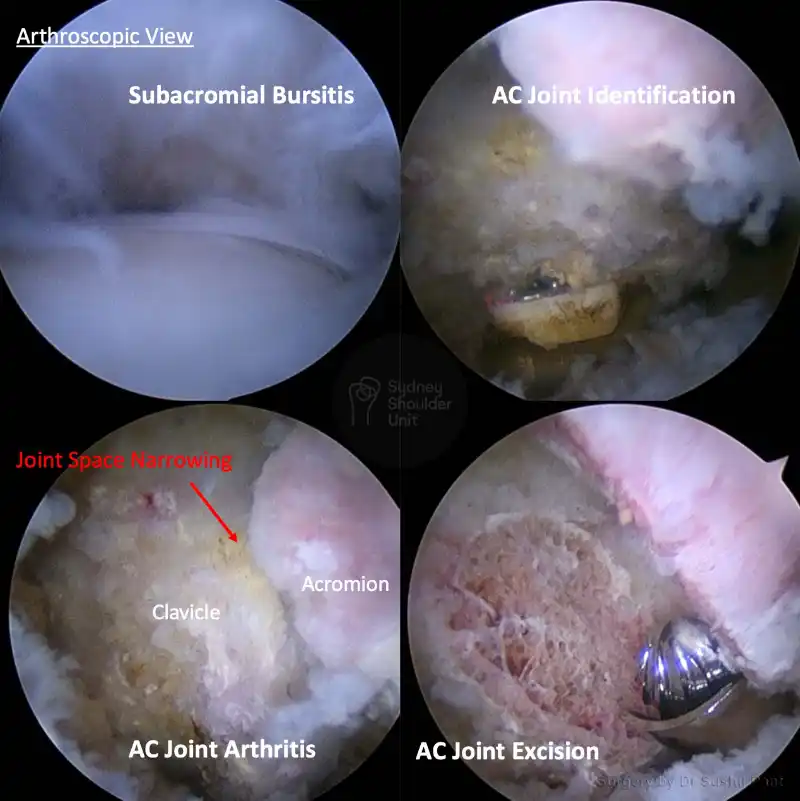
This 48 year old gentleman presented with pain over the top of his shoulder over many months. A diagnosis of AC Joint arthritis was made and he responded well to an ultrasound guided cortisone injection initially. However, that wore off over a few months and he was unable to sleep on the affected shoulder and very keen to get back to his active lifestyle, so he elected to proceed with surgery.
He underwent an Arthroscopic Acromioclavicular Joint (ACJ) excision via 3 small keyhole incisions. His procedure was routine, he stayed overnight in hospital, and was discharged home the following morning with oral painkillers.
He commenced immediate range of motion and discarded his sling between 1 -2 weeks after surgery. At three months, he is back to the gym and kayaking and is happy with his outcome; his keyhole incisions were only barely visible at the 3 month follow up.
Arthroscopic AC Joint excision is a very successful operation when non-surgical measures have been exhausted.
This 53 year old lady presented with right-sided shoulder pain after injuring her shoulder at work. She underwent a period of rest, cortisone injection and 3 months of physiotherapy without improvement.
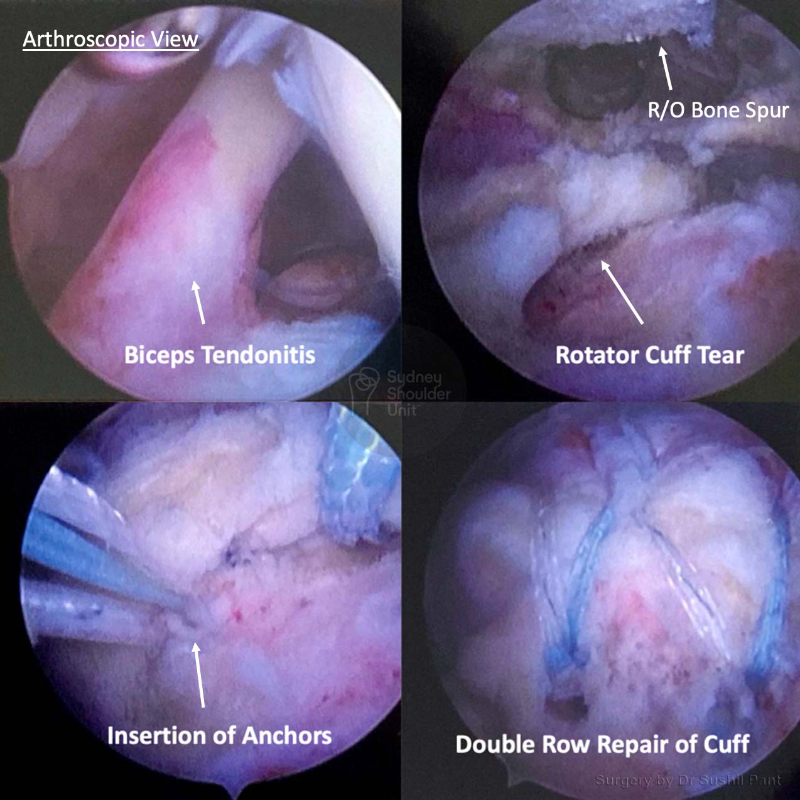
After a careful history and examination, an MRI scan was undertaken. The MRI showed a Rotator Cuff Tear with Biceps Tendonitis.
The images taken at surgery (key-hole) demonstrate significant biceps tendonitis with inflammation and thickening of the tendon. The biceps tendon was taken out of the shoulder joint and re-anchored under the arm-pit (biceps tenodesis). The bursitis and bone spur was cleaned out and the rotator cuff tear was repaired with 4 anchors with good compression of the tendon foot-print.
She was discharged home the following day after surgery and placed in a sling for six weeks. She underwent JPL rehab which commenced at two weeks post-surgery. Strengthening commenced at months under the guidance of her physiotherapist.
She no longer has her previous shoulder pain and has good power of her rotator cuff.
Enquiries between 8am-6pm (Mon-Fri) will be responded to within 30-60 minutes.
"*" indicates required fields
Alternatively, if you have any further questions or would like a consultation with Dr Pant get in touch:

1. Medicare Number
2. Position on card
3. Expiry Date