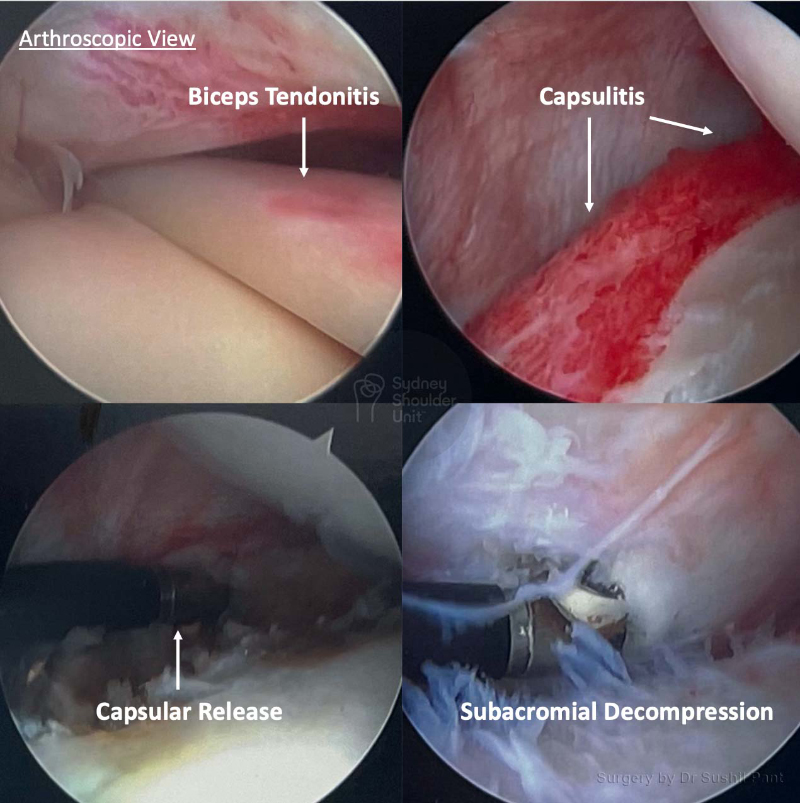
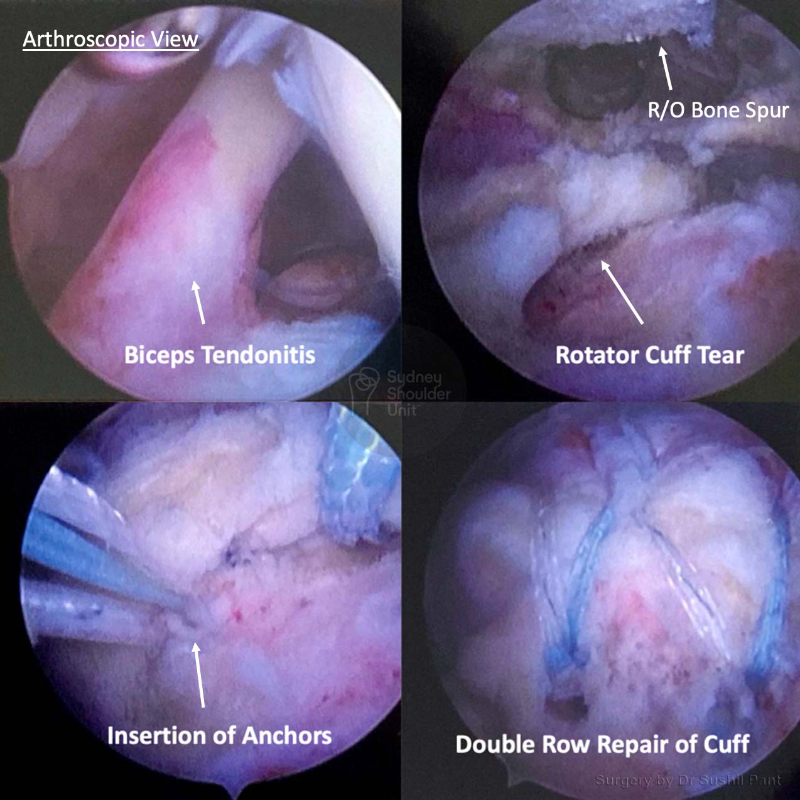
Biceps tendonitis is inflammation or irritation of the upper biceps tendon near the front of your shoulder. Also referred to as the “long head of the biceps tendon” (LHBT), this tendon is a strong cord-like structure that connects the biceps muscle to the top of the shoulder socket.
A common presentation of biceps tendonitis is pain at the front of the shoulder and weakness with certain shoulder movements. This is because the biceps tendon runs in a very narrow groove at the front and with inflammation may thicken and become irritated or even compressed. The biceps tendon normally glides about 2 cm during overhead shoulder movement.
In the early stages, the tendon becomes inflamed and swollen. With ongoing tendonitis, the tendon sheath (covering) can thicken, and eventually, the tendon itself may enlarge and become double or triple the size of a normal tendon. This enlarged tendon can be a source of pain over the front of the shoulder.
In some cases, the biceps tendon may tear (partial or complete). A complete tear will result in tendon rupture and loss of contour about the front of the arm, this is referred to as a “Popeye” sign.