
Frozen shoulder arthroscopic release is a minimally invasive keyhole procedure to treat frozen shoulder. It is also referred to as a capsular release – as the tight/inflamed capsule in the shoulder joint is released during surgery. It is often done as a part of other keyhole procedures in the shoulder, such as a subacromial decompression, biceps tenodesis and/or rotator cuff repair.
After an isolated frozen shoulder arthroscopic release a sling is worn for 1-2 weeks, and JPL therapy commences immediately after surgery. Strengthening is allowed at 4-6 weeks, and full unrestricted activity is possible at 6-12 weeks after surgery. This pathway is modified if other procedures are carried out at the same time.
This is a keyhole procedure that uses cameras and small instruments inside the shoulder to release the tight shoulder joint capsule to improve range of motion; and treat any other pain generators in the shoulder at the same time.
Physiotherapy is commenced immediately after surgery and the procedure can be done as a day stay or with an overnight admission.
Most patients improve without surgery over 6-12 months. Surgery is suitable for those patients who are not responding to non-surgical treatments and find that:
If your symptoms have persisted for six months and your condition is deteriorating then surgery is a good option (particularly for the younger patient).
There are three essential components to a good outcome from surgery
Dr Pant utilises the JPL pathway for most patients and this will form the basis of your rehabilitation after surgery.
The JPL pathway allows for self-directed, early passive shoulder range of movement:
A sling may be worn for up to 6 weeks after your surgery. However, after a frozen shoulder release, Dr Pant will encourage you to come out of the sling as much as possible – to commence immediate physiotherapy and minimise re-scarring (re-freezing) your shoulder joint capsule.
Surgery is a carefully choreographed process and you are being treated by a sub-specialist shoulder surgeon and a highly experienced team; however, all surgeries inherently carry some risk of complications.
The risk of complications after Frozen Shoulder release surgery are less than 1% in the Sydney Shoulder Unit experience.
Patients who smoke, use tobacco products, have diabetes, or elderly are at higher risk of complications both during and after surgery. They are also more likely to have problems with wound and bone healing.
With careful patient selection, surgical release and consistent physiotherapy patients report improved range of motion and less pain. Range of motion will improve with both forward elevation and external rotation. In a small number of patients the capsule may rescar and become stiff, requiring a second keyhole release.

Dr Sushil Pant is a leading Australian trained orthopaedic shoulder surgeon. He is the founder and medical director of the Sydney Shoulder Unit; and is a Shoulder Surgeon at Sydney Sports Medicine Centre at Sydney Olympic Park.
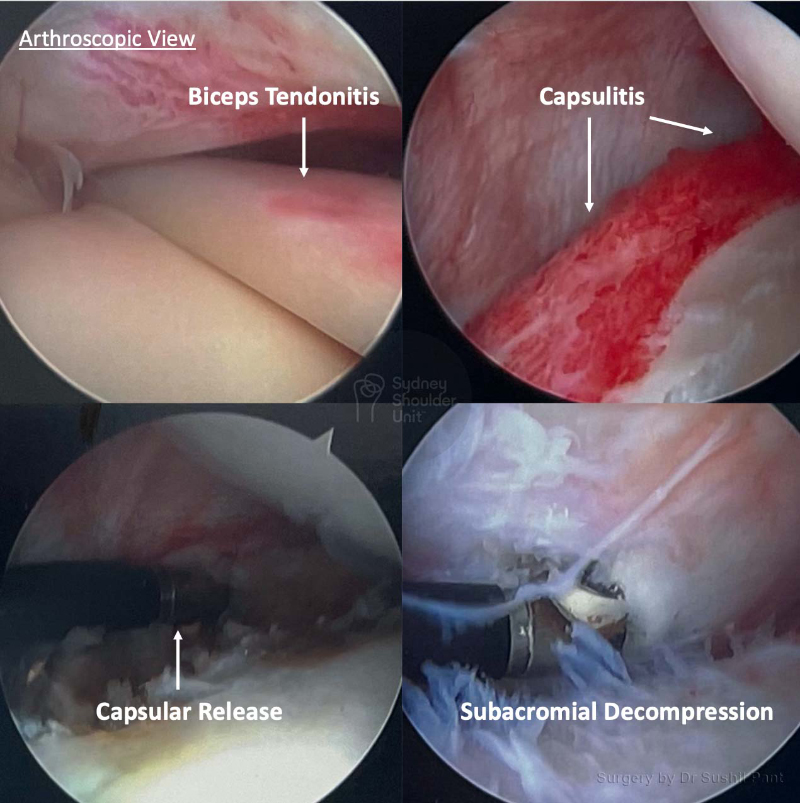
This gentleman in his 60s suffered from a frozen shoulder for almost a year; his symptoms were unrelenting and he failed to improve over time despite non-surgical treatment. Examination and MRI imaging confirmed ongoing frozen shoulder as well as biceps tendonitis, subacromial bursitis, and AC joint arthritis; thankfully his rotator cuff was intact.
He underwent arthroscopic frozen shoulder surgery (capsular release) and a biceps tenodesis, subacromial decompression and excision of his AC joint. Range of motion exercises were commenced immediately after surgery using the JPL protocol.
Enquiries between 8am-6pm (Mon-Fri) will be responded to within 30-60 minutes.
"*" indicates required fields
Alternatively, if you have any further questions or would like a consultation with Dr Pant get in touch:

1. Medicare Number
2. Position on card
3. Expiry Date