Surgical fixation is reserved for more complex cases such as fractures with displacement (fracture fragments shifted out of position), high demand patients (overhead workers, high-level athletes), or those that are unable to cope with the pain or loss of function.
Dr Pant has extensive experience treating proximal humerus fractures and is highly skilled in the surgical repair of all shoulder fractures should that be required. As the lead shoulder trauma surgeon at St Vincent’s Hospital for many years, he has experience with a vast array of shoulder trauma cases and is well versed in guiding you to full recovery.
These are the factors when considering surgery:
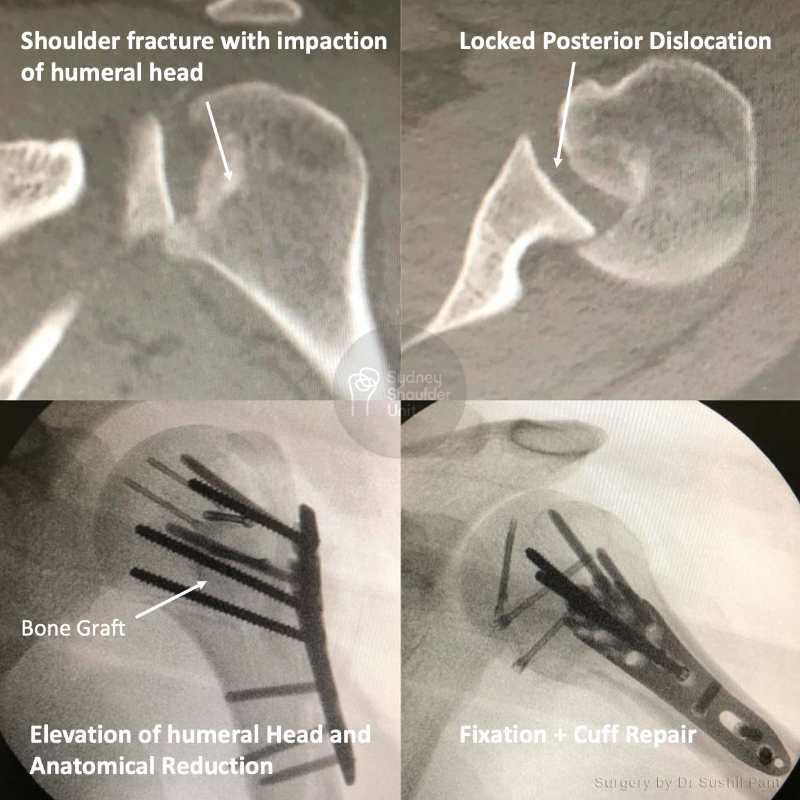
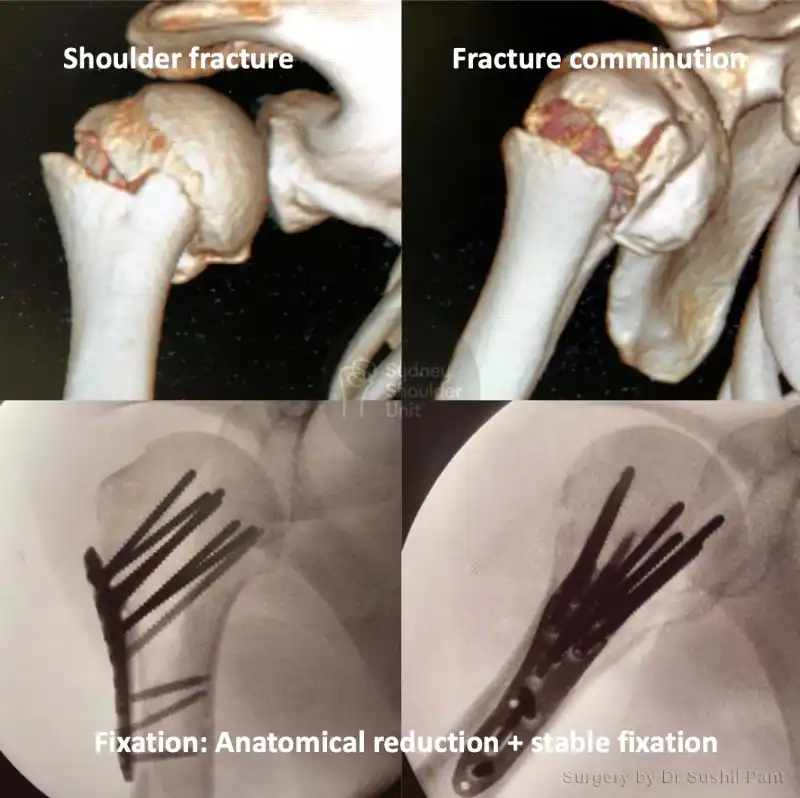
1. Fracture displacement
If the fracture fragments are too far apart then they may heal in the wrong position; once the fracture has healed it is often very difficult to “re-break” and “reset” them in the correct position. Abnormal fracture position may result in reduced shoulder function.
After the first 2-4 weeks, the fracture will start to heal and will become difficult to mobilise and fix accurately.
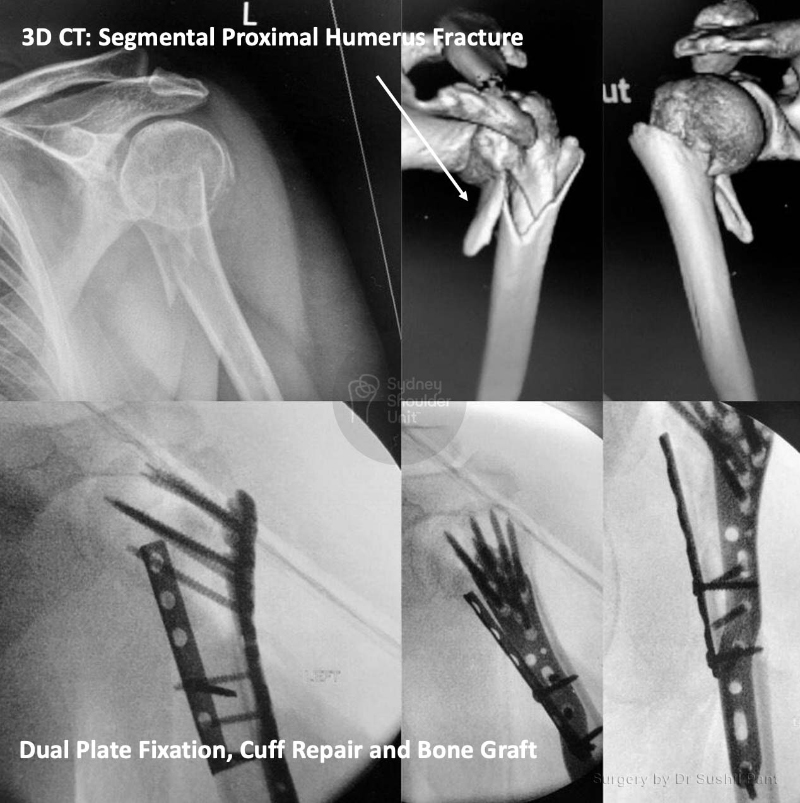
2. Tuberosity and Rotator cuff involvement
If the tuberosities (rotator cuff attachment points on the humeral head) have pulled away more than 5-10mm then you may benefit from surgery. These fragments have a constant deforming force and will usually continue to move further away (over days to weeks) while the fracture is healing.
3. High-level athletes
In these cases, surgery is a better option early to allow faster recovery and more reliable outcomes. Tuberosity displacement is accepted up to 3mm.
4. Overhead work
Those patients who depend on overhead function at work may benefit from earlier surgery to minimise the time in a sling, shoulder stiffness, and enhance their ability to undertake work overhead.
5. Other issues
Some patients may live alone, be a carer for their significant other, be unable to tolerate six weeks in a sling, or unable to manage their pain – in such cases it is appropriate to consider surgical repair to allow more predictable and faster recovery.