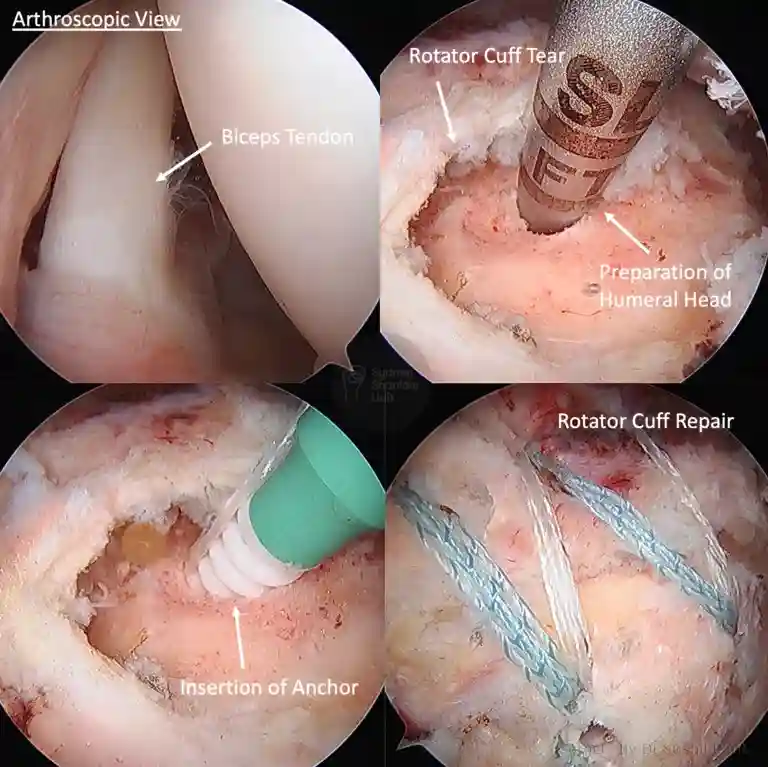
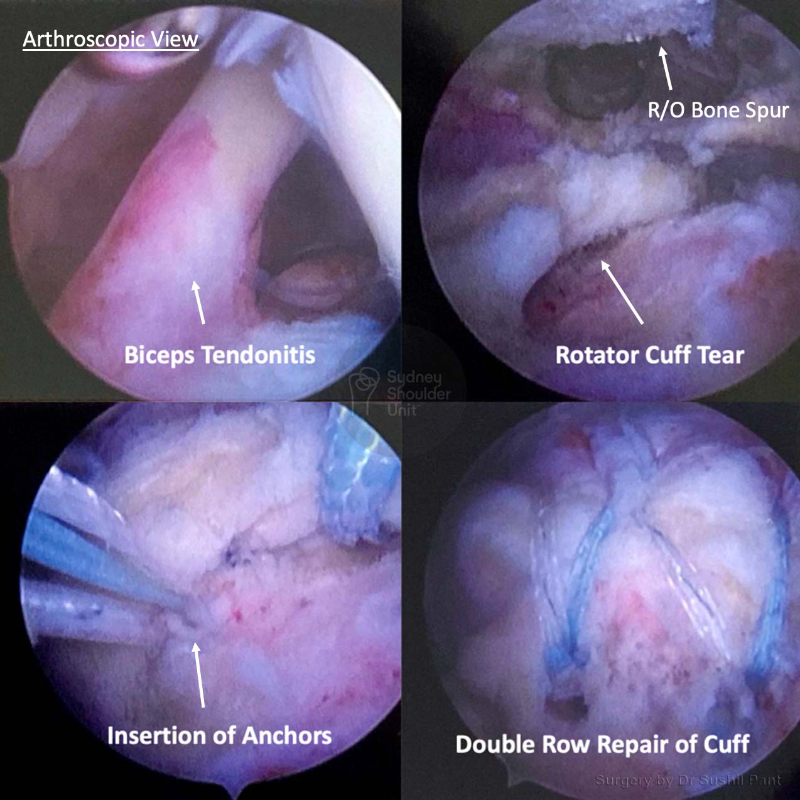
The principle of arthroscopic rotator cuff surgery is to reattach the torn tendon back to the humerus (ball) and address any other areas of concern at the same time – biceps tendon, shoulder spur, bursitis, acromioclavicular joint, and shoulder joint capsule. The procedure is almost always carried arthroscopically (keyhole) and involves an overnight stay in hospital. Patients are in a sling for six weeks and start rehabilitation using the JPL protocol at two weeks post-surgery.

The procedure is performed under a General Anaesthetic where you will be positioned on your side and the affected arm secured in a special arm holder.
Biceps
Bone Spur and Bursa
Rotator Cuff Tear
AC Joint Resection


There are three essential components to a good outcome from surgery:
Post-operative physiotherapy
Dr Pant utilises the JPL pathway for most patients and this will form the basis of your rehabilitation after surgery; it will be modified to suit your individual circumstance.
The JPL pathway allows for self-directed, early passive shoulder range of movement:
Therapy overview
After the surgery you will be in a sling and protect your shoulder to allow the rotator cuff repair to heal. At two weeks after the surgery, Dr Pant will see you at your review appointment and discuss the JPL rehabilitation protocol with you. This JPL physiotherapy protocol will commence two weeks after your surgery.
The therapy program will focus on flexibility and range of motion exercises initially. These gentle stretches will improve your range of motion and prevent shoulder stiffness. As the rotator cuff repair begins to heal you will be able to progress to exercises that strengthen your shoulder muscles. Shoulder strengthening is commenced at 12 weeks post rotator cuff repair surgery.
Sling
A sling is required for the first 6 weeks after your surgery; the sling is worn for a further 6 weeks outside of the house (to remind others you have had shoulder surgery). In some instances you may only need a sling for 1-2 weeks – Dr Pant will discuss these cases with you.
The type of sling is selected specific to you and your shoulder surgery:

Driving after shoulder surgery
Showering and getting dressed
Sleeping after Shoulder Surgery
Elbow and hand movement