Patients often present with shoulder pain and a reduced range of motion.
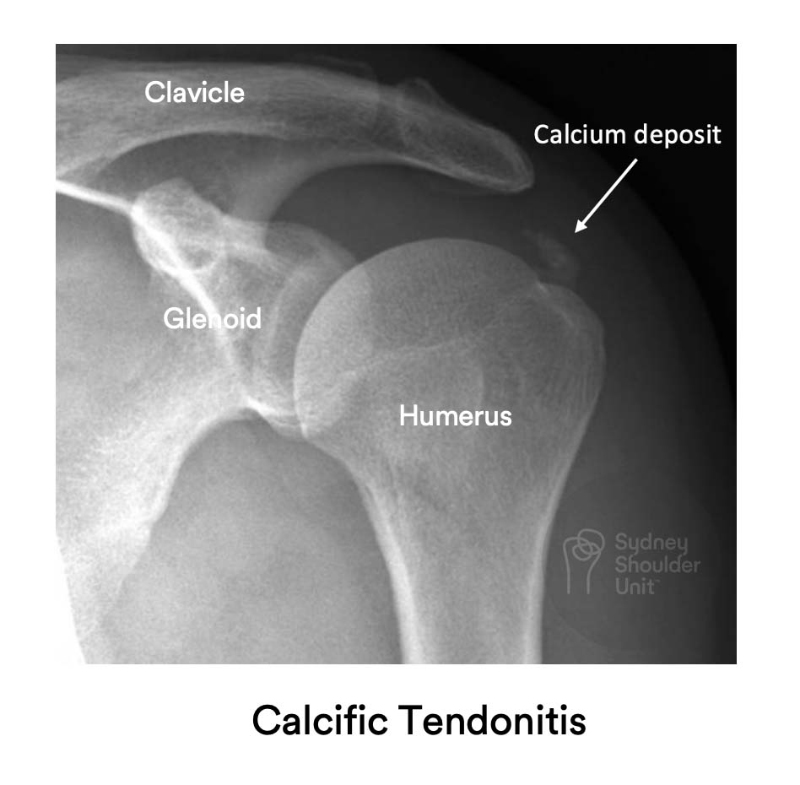
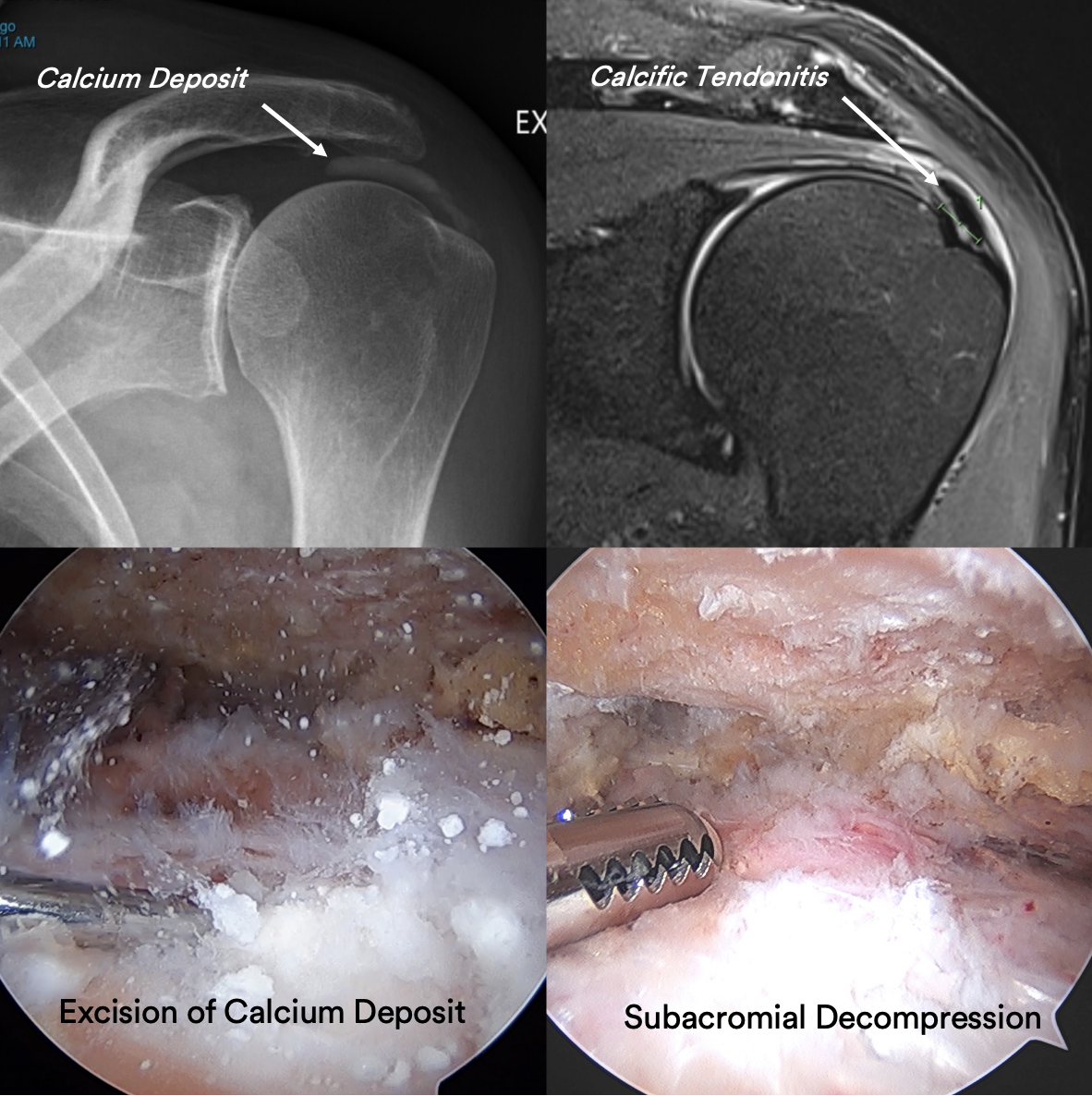
The diagnosis is often made with a plain x-ray where a calcium deposit may be seen above the tendon insertion. In some cases, it is prudent to obtain an MRI scan to exclude a rotator cuff tear or other pathologies about the shoulder. A supraspinatus tendon tear is not uncommonly associated with calcific tendonitis.