Frozen shoulder (also referred to as adhesive capsulitis) presents with pain and stiffness in the shoulder; often without any trauma or incident.
In a frozen shoulder, the shoulder capsule thickens and becomes stiff and tight. The thick bands of tissue (adhesions) develop within the shoulder joint limiting movement.
The classical presentation of frozen shoulder is initially intense pain and then progressively being unable to move your arm. Often there is no history of trauma or any other illness.

Freezing
Frozen
Thawing
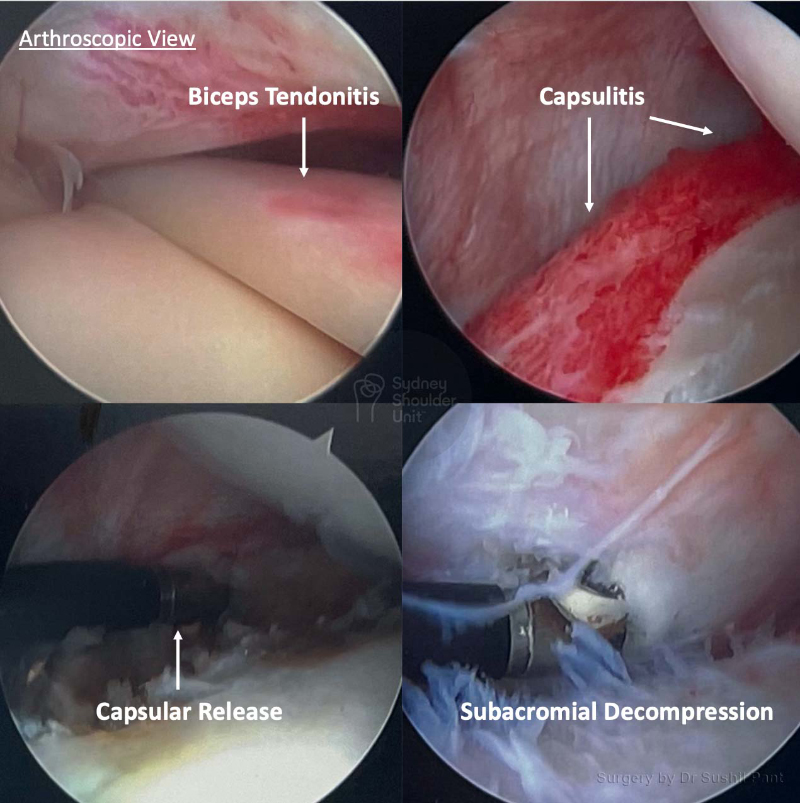
Frozen shoulder surgery is reserved for patients whose range of motion is going backwards at 6-9 months into a frozen shoulder. It is also suitable for those who are found to have a time urgent issue on the MRI scan (such as an acute rotator cuff tear or biceps tendon dislocation).