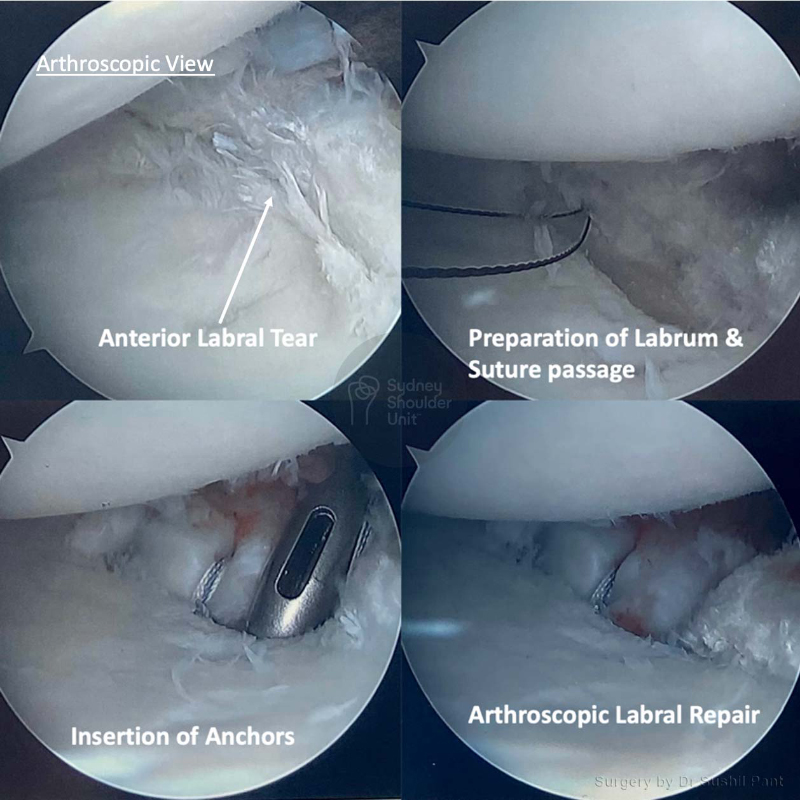
An arthroscopic labral repair is a surgical procedure where small keyhole incisions are used to access the shoulder using specialised instruments. For most patients who sustain shoulder dislocations that require a labral repair, we are able to undertake this utilising an arthroscopic technique.
Using a minimally invasive approach means faster recovery time, minimal blood loss, and fewer complications from surgery. Arthroscopic labral repair is a common procedure and is done either as a day only case or with an overnight stay in hospital. The results are excellent and most patients return to their previous level of function.



Watch a surgical animation demonstrating how Dr Pant performs a Shoulder Labrum Repair to fix shoulder dislocations.
There are three essential components to a good outcome from surgery:
Post-operative physiotherapy
Dr Pant utilises the JPL pathway for most patients and this will form the basis of your rehabilitation after surgery; it will be modified to suit your individual circumstance.
The JPL pathway allows for self-directed, early passive shoulder range of movement:
Therapy overview
After the surgery you will be in a sling and protect your shoulder to allow the labral repair to heal. At two weeks after the surgery Dr Pant will see you at your review appointment and discuss the JPL rehabilitation protocol with you. This JPL physiotherapy protocol will commence two weeks after your surgery.
The therapy program will focus on flexibility and range of motion exercises initially. These gentle stretches will improve your range of motion and prevent shoulder stiffness. As the labral repair begins to heal you will be able to progress to exercises that strengthen your shoulder muscles. Shoulder strengthening is commenced at 12 weeks post labral repair surgery.
Sling
The type of sling is selected specific to you and your shoulder surgery

When can I drive?
Showering and getting dressed
Sleeping after Shoulder Surgery
Elbow and hand movement