
Rotator cuff tendon tears usually occur in middle age, around 40-60 – either due to a new injury (acute), wear and tear over time (chronic), or a combination of both (acute on chronic). Supraspinatus tendon tear is the most common; and the most urgent is a subscapularis tendon tear or a very large acute tendon tear.
Patients usually present with pain over the side of the shoulder, weakness of shoulder function, difficulty undertaking tasks overhead, and trouble sleeping on the affected side.
Rotator cuff tendon tears may occur with other conditions in the shoulder and therefore it requires careful workup and investigation to exclude subacromial bursitis, shoulder spurs, shoulder impingement, biceps tendonitis, biceps tendon tears, SLAP tears, and AC joint arthritis.
The rotator cuff is a group of four muscles that come together as tendons and surround the shoulder joint; they envelope the humeral head almost circumferentially. The rotator cuff attaches the humerus to the shoulder blade and thus helps lift and rotate your arm.
Under the roof of the shoulder (acromion) there is a lubricating sac called a brusa – this brusa sits between the rotator cuff and the acromion. The brusa allows the rotator cuff to glide and move freely when you move your arm. When the rotator cuff tendons are injured or damaged, the bursa may also become inflamed, thickened and painful.

A rotator cuff tear is a common cause of pain and disability in adults – especially in middle age. A rotator cuff tear will weaken your shoulder and make activities of daily living difficult – such as combing your hair, getting dressed, driving and much more.
When one or more of the rotator cuff tendons is torn, the tendon is no longer fully attached to the humerus. Most tears occur in the supraspinatus tendon, but other parts of the rotator cuff may also be involved. In the early stages, the tendon begins to fray, then as the damage progresses the tendon may completely tear (this may sometimes happen when lifting something heavy at home, work or the gym).
Partial Rotator Cuff Tear
Full-thickness Rotator Cuff Tear


There are two main causes of rotator cuff tears: injury/fall/trauma (“acute”) and degeneration/wear and tear (“chronic”); in some cases, it may be a combination of both.
These are usually degenerative tears and happen slowly over time (often unnoticed). Patients are usually older (>65 years old). They may be:
As we age, the blood supply to the tendon insertion lessens. Without a good blood supply, the body’s natural ability to repair tendon damage is reduced, thus increasing the chance of tear formation and progression.
As we age bone spurs (bone overgrowth) often develops on the undersurface of the acromion bone (roof of the shoulder). When we lift our arms, the spurs rub on the rotator cuff tendon. The combination of an inflamed bursa and bone spurs leads to “shoulder impingement” syndrome. Over time this may weaken the tendon and lead to rotator cuff tendon tears.
General inflammatory conditions (such as Rheumatoid arthritis) will cause inflammation of tendons and joints. In the shoulder this will increase the chance of rotator cuff tendon wear and tear, thus leading to degenerative rotator cuff tears over time.
Calcium deposit in the rotator cuff tendon may degrade the tendon over time and lead to a rotator cuff tear.
Once the rotator cuff tendon tear process has begun it will not heal itself. The tendon ends often have poor blood supply and the quality of the torn ends also begins to deteriorate (tendinosis). In most cases the tear will progress over time – how fast the tear progresses depends on many factors.
It is important to study the tear carefully on MRI to assess the nature of the tear pattern and the quality of the tendons and muscles – this will guide treatment.
The rotator cuff tear is assessed for:
How fast the tear progresses depends on a number of factors:
The most common symptoms of a rotator cuff tear include:
Generally speaking, acute tears (from a fall or trauma) usually cause intense pain. Some patients report a snapping sensation followed by immediate shoulder weakness.
Tears that develop slowly over time due to overuse may also eventually lead to shoulder pain and arm weakness. Patients may report shoulder or arm pain when lifting the arm, and this pain may move down the arm. Initially, the pain may be mild and only with activity; over time the pain may occur at rest and even at night – waking patients up from sleep and making it difficult to sleep on the affected side. In the initial stages painkillers, activity modification, therapy may settle the symptoms. As the condition progresses, the symptoms persist despite maximising treatment.
Some rotator cuff tears are not painful and may present with weakness and/or loss of function.
Examination
Rotator cuff tears may occur in isolation or with other conditions in the shoulder. A careful history will provide initial clues to other possible diagnoses. The examination focuses on identifying areas of tenderness on palpation – in particular the acromioclavicular joint, biceps tendon, glenohumeral joint (shoulder joint), and the subacromial space (area directly above the tendon). It is important to carefully assess the range of motion about the shoulder joint. Each of the rotator cuff tendons should be carefully examined for integrity and power. Special tests then are used to isolate areas of concern to identify all relevant conditions that coexist.
In some cases, there may be an overlapping syndrome from a “pinched” nerve in the neck that can refer to pain to the shoulder.
Imaging
X-ray: this is the first test to be performed and provides an overall assessment of the shoulder joint; it may show evidence of acromioclavicular joint arthritis, bone spurs, rotator cuff insertion problems, and shoulder joint arthritis.
Ultrasound: this is an easy test to obtain and can be useful; however this test is often very much dependent on the person performing the scan to identify areas of concern.
MRI: This is the most valuable scan when investigating possible rotator cuff tendon conditions. It shows the soft tissues, tendons, muscles, bursa, and shoulder joint in great detail. The rotator cuff tear location, size, muscle quality, tendon quality, degree of retraction can all be assessed with high accuracy. It will also allow assessment of the bursa, shoulder spur, biceps tendon, acromioclavicular joint and shoulder joints in detail.
Assessment of the muscle/tendon quality will help in deciding whether this is a “new” or “old” tear and what treatment options are suitable.
The key factors when deciding on treatment for a rotator cuff tear are:
Generally speaking, if you have a rotator cuff tear and you keep using your shoulder, despite increasing pain, you may cause further damage. Rotator cuff tears tend to get larger over time, especially with increased use.
If you have shoulder pain that is not settling then you should see your doctor and/or Orthopaedic shoulder surgeon sooner.
The non-surgical treatment options may include:
Physiotherapy
Guided physiotherapy is useful to restore range of motion, strength, capsular stretching, scapular (shoulder blade) stabilising and a deltoid strengthening program. Strengthening the muscles that support your shoulder, shoulder blade and upper back may relieve pain and prevent further injury.
Cortisone injection
If rest, activity modification, medications, and physiotherapy do not settle your symptoms then a guided subacromial cortisone (steroid) injection by the radiologist is a good option. The duration for which it provides relief is variable and not all patients will respond to this. Usually, a maximum of two to three injections per year is recommended.
The main advantage of non-surgical treatment is that it avoids the major risks of surgery, such as:
The disadvantage of non-surgical treatment are:
Surgery is recommended if you have exhausted non-surgical treatment or are deemed to have a “high” risk cuff tear from the initial diagnosis.
Generally speaking, these patients should seek surgical repair:
The principle of rotator cuff surgery is to reattach the torn tendon back to the humerus (ball) and address any other areas of concern at the same time – biceps tendon, shoulder spur, bursitis, acromioclavicular joint, and shoulder joint capsule. The procedure is almost always carried arthroscopically (keyhole) and involves an overnight stay in hospital. Patients are in a sling for six weeks and start rehabilitation using the JPL protocol at two weeks post-surgery.
The key point is to remember which conditions in your shoulder are “time urgent” and which are not. Dr Pant will clearly outline this for you during your consultation.
If you are unable to undertake basic tasks or to look after yourself, unable to drive, unable to get dressed, or have difficulty with hygiene and toileting.
Most rotator cuff tears are caused by normal wear and tear that occurs with aging; so it is difficult to prevent these types of “degenerative” tears. However, “acute” tears may be minimised by physiotherapy and shoulder strengthening programs. As we get older, doing “closed” chain is preferred to “open chain” exercises.
The other risk factors for a rotator cuff tears are repetitive lifting or overhead activities. Athletes and sports that require repeated overhead activity (such as tennis and weightlifting) are at particular risk. Those whose work required manual work overhead such as painters and carpenters are also at risk.

Dr Sushil Pant is a leading Australian trained orthopaedic shoulder surgeon. He is the founder and medical director of the Sydney Shoulder Unit; and is a Shoulder Surgeon at Sydney Sports Medicine Centre at Sydney Olympic Park.
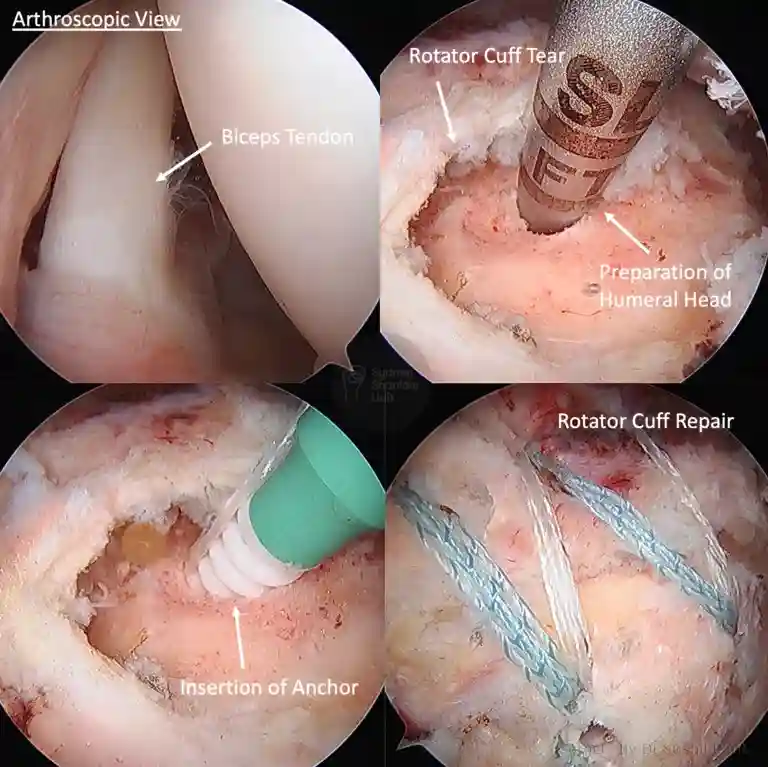
This 48 year old gentleman works as a metal fabricator and presented with several months of new shoulder pain; he was finding it difficult to undertake overhead work and was limited with daily activity around the house.
MRI scans demonstrated a large rotator cuff tear with biceps tendonitis. Given the tear size and limitation in function – he proceeded with surgery.
He underwent keyhole shoulder surgery to re-anchor the biceps tendon (biceps tenodesis) and repair the rotator cuff (double row repair). An excellent repair was obtained with restoration of the anatomical footprint.
He commenced JPL rehabilitation at 2 weeks post-operatively; and an abduction sling was worn for six weeks in total. Strengthening commenced at 3 months post-surgery.
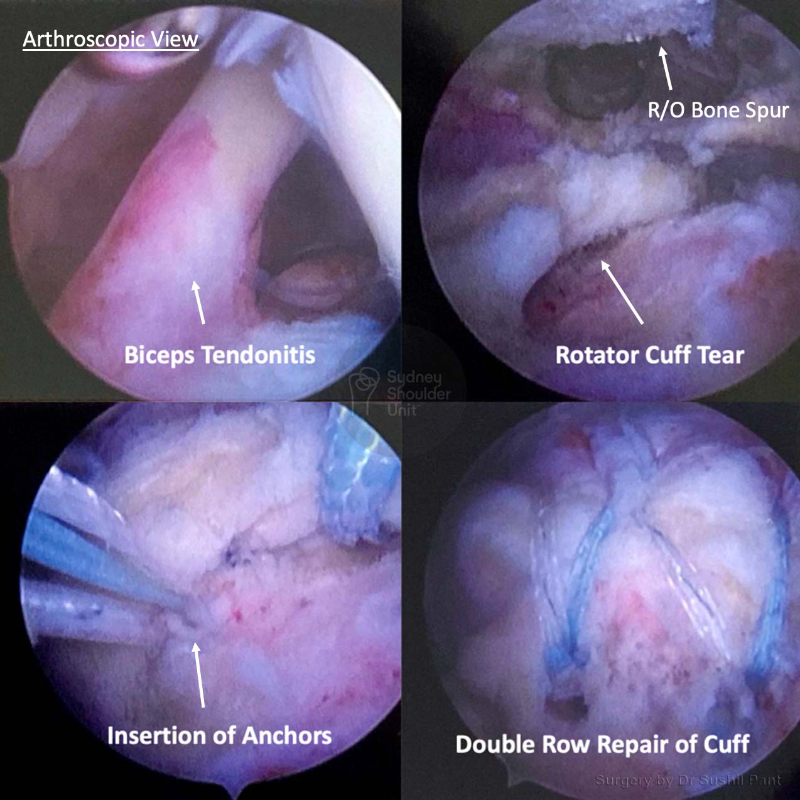
This 53 year old lady presented with right-sided shoulder pain after injuring her shoulder at work. She underwent a period of rest, cortisone injection and 3 months of physiotherapy without improvement.
After a careful history and examination, an MRI scan was undertaken. The MRI showed a Rotator Cuff Tear with Biceps Tendonitis.
The images taken at surgery (key-hole) demonstrate significant biceps tendonitis with inflammation and thickening of the tendon. The biceps tendon was taken out of the shoulder joint and re-anchored under the arm-pit (biceps tenodesis). The bursitis and bone spur was cleaned out and the rotator cuff tear was repaired with 4 anchors with good compression of the tendon foot-print.
She was discharged home the following day after surgery and placed in a sling for six weeks. She underwent JPL rehab which commenced at two weeks post-surgery. Strengthening commenced at months under the guidance of her physiotherapist.
She no longer has her previous shoulder pain and has good power of her rotator cuff.
Enquiries between 8am-6pm (Mon-Fri) will be responded to within 30-60 minutes.
"*" indicates required fields
Alternatively, if you have any further questions or would like a consultation with Dr Pant get in touch:

1. Medicare Number
2. Position on card
3. Expiry Date