There are two main joints that may be affected by arthritis. The first is the acromioclavicular (AC) joint – where the end of the collarbone (clavicle) meets the roof the shoulder (acromion). The other is where the head of the humerus (ball) fits into the glenoid (shoulder blade socket) – this is called the glenohumeral joint.
When we generally speak about shoulder arthritis – it usually refers to “glenohumeral” joint arthritis.
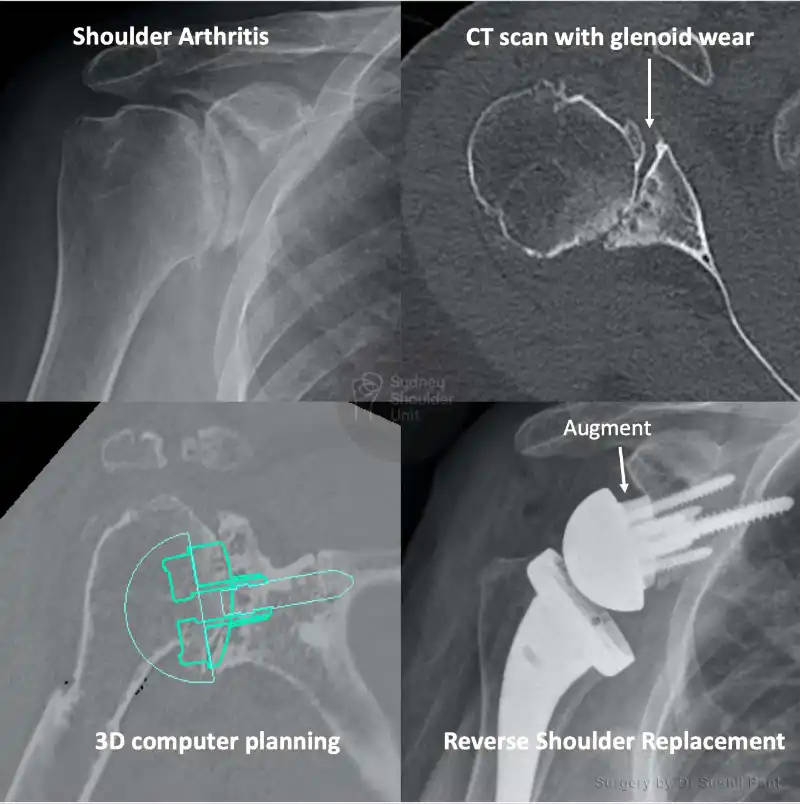
Arthritis refers to a condition where the cartilage covering the surface of a joint wears away, this causes bone-bone contact which leads to loss of movement and pain.
The shoulder joint is surrounded by the rotator cuff muscles (four in total) and the deltoid muscle which functions to move the shoulder joint.
As we age the quality of the cartilage and tendons may degenerate leading to pain, stiffness and weakness of the shoulder joint.

Osteoarthritis
This is most common form of arthritis in the shoulder
It is also called “wear and tear” arthritis and this condition that destroys smooth outer covering of bone (as it forms a joint) – this is the articular cartilage. As the articular cartilage wears away the protective space between bones narrows and the bones of the joint rub against each other, causing pain. This is referred to as “bone on bone” arthritis. Osteoarthritis typically affect those over the age of 55
Rheumatoid Arthritis
Rheumatoid arthritis is a systemic inflammatory condition that affects the bones, tendons and joints. This chronic condition may affect multiple joints in the body. Uniquely Rheumatoid arthritis affects the synovium, the lining that covers all joints in the body which lubricates the joint and makes it easier to move. The synovium becomes thickened and inflamed and this leads to pain and swelling of the joint. Over time the inflammation will start to attack the articular cartilage
Rheumatoid arthritis is an autoimmune condition – which means that the immune system attacks its own tissues.
More recently medication (DMARDs) used to treat Rheumatoid arthritis have become advanced and this has meant that the rate of joint involvement has dropped markedly.
Posttraumatic arthritis
This is a form of osteoarthritis that develops after injury, such as a shoulder fracture or dislocation. It usually takes many years to develop after the initial trauma. Patients who develop posttraumatic arthritis tend to be younger, usually 40-50 year olds.
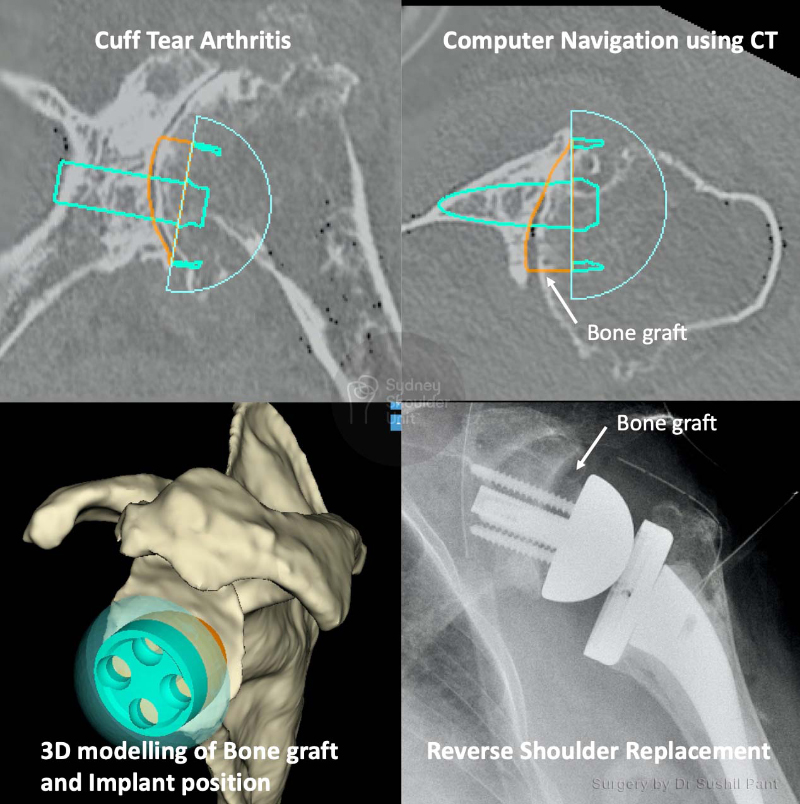
Rotator Cuff Tear Arthritis
Arthritis may also develop due to long-standing rotator cuff tendon tears. As the tendon tear becomes large, retracts and is irreparable the shoulder joint is no longer held in place and the ball moves up and out of the socket to sit under the acromion. This will lead to cartilage damage in the joint over time and is referred to as cuff tear arthropathy (arthritis).
The pain from arthritis (bone on bone) and loss of rotator cuff tendon function can render the arm very painful and without function – at the end stages it looks clinically like shoulder paralysis (referred to as pseudoparalysis).
Avascular Necrosis
Avascular necrosis (AVN) occurs when the blood supply to the humeral head is disrupted (that is it becomes avascular) and this causes bone cells to die (referred to as necrosis).
AVN progresses through stages – with progressive more bone death, cartilage damage, and joint collapse.
Initially, AVN starts off affecting the humeral head (ball) and over time it may also affect the glenoid (socket). The causes of AVN are:

As with most arthritic conditions, the initial treatment is almost always non-surgical. The principles of non-surgical treatment are:
Rest and activity modification
You may need a short period of rest and/or change the way you use your arm to limit activities that exacerbate shoulder pain.
Analgesia
Non-steroidal anti-inflammatory (NSAIDs) and paracetamol are a good start to controlling baseline pain. Long-acting pain killers overnight can be useful. Prolonged use of NSAIDs may irritate the stomach lining and lead to gastric ulcers – therefore they should be used for short periods under the guidance of your local doctor.
Physiotherapy
Both self-directed and guided physical therapy is useful to keep the shoulder joint supple and strengthen the rotator cuff, scapula stabilising, upper back and deltoid muscles. This may offload the arthritis pain made worse by muscle imbalance.
Cortisone injections
Cortisone injections when used correctly can dramatically reduce inflammation and arthritis pain. However, this is not a cure and the effect is generally temporary. No more than two injections are recommended per year. A plain X-ray of the shoulder should always be obtained prior to cortisone injection into the joint – as cortisone itself is associated with avascular necrosis (AVN) of the shoulder joint – and this needs to be excluded prior to the injection.
General health optimisation
Seeing your general practitioner and optimising your cardiovascular health, diabetes, blood pressure, and diet can all lead to improvement in overall health. It also makes you a better anaesthetic and surgical candidate should you require future surgery.
If your shoulder arthritis symptoms are not responding to non-surgical treatment then there are a number of surgical options:
Arthroscopy
In cases of mild shoulder arthritis, arthroscopic (keyhole) shoulder surgery may be used to target pain generators in the shoulder. These include:
Arthroscopy will not eliminate arthritis, but treat areas that may be exacerbating your shoulder pain; this will delay the need for shoulder replacement surgery.
Joint Replacement
Anatomical shoulder replacement
Reverse Shoulder Replacement