The Shoulder is the most mobile joint in the body. This allows you great function but increased risk of dislocations. When the shoulder dislocates, the Labrum (ring of cartilage) around the glenoid (socket) may tear.
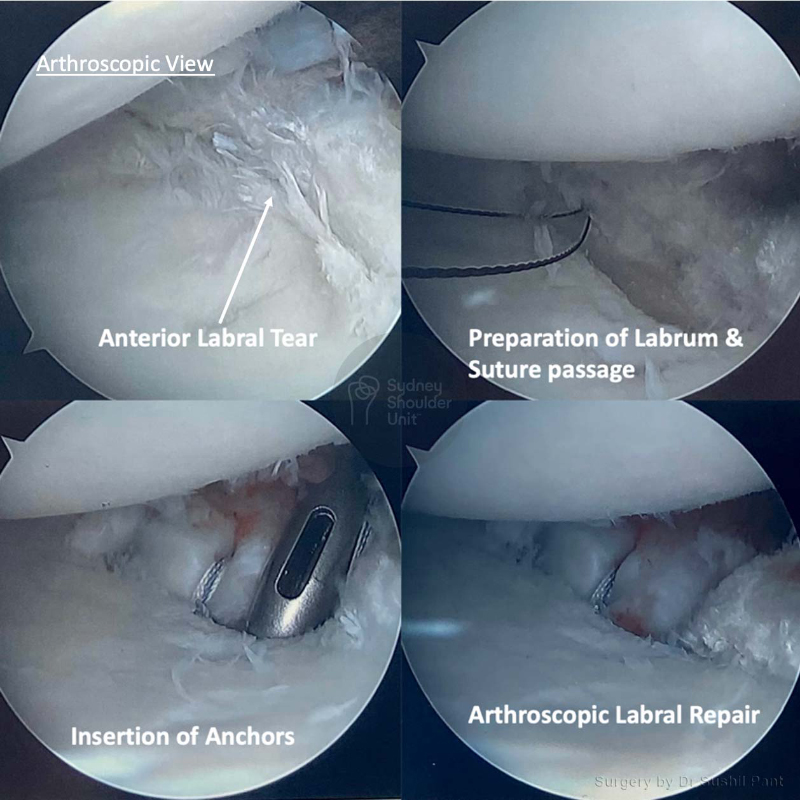
The Labrum is a soft tissue ring around the glenoid (socket) that deepens the shoulder joint and keeps the humeral head (ball) in the joint. After shoulder dislocations (especially recurrent episodes) the Labrum may tear off the socket and no longer function in stabilising the shoulder joint.
The labrum can tear at the:

Once a shoulder has dislocated, it is prone to repeat episodes. When the shoulder is loose and slips out of place repeatedly over a period of time, it is called chronic shoulder instability.
With shoulder instability you may have a “partial dislocation” – also called a “subluxation”; or the joint may come entirely out of the socket and result in a “complete dislocation”. Both partial and complete dislocations may result in pain and unsteadiness of the shoulder joint.
Shoulder instability may be in one direction (unidirectional) or in more than one direction (multidirectional). If it is unidirectional, it can be out the front (anterior) or the back (posterior); 95% of cases are unidirectional and anterior (out the front).
Dr Pant will take a careful history, examine your shoulder and then assess your imaging to make a diagnosis and assess the severity of your shoulder dislocation.
This will focus on your age at first dislocation, hand dominance, type and level of sport participation, overhead contact, number of instability episodes and frequency, family history and other related issues. Dr Pant will take time to understand your particular citation and your goals and expectations; shoulder instability affects each individual differently and it is important to personalise treatment.
The examination will involve careful inspection and palpation for areas of tenderness; Dr Pant will then check your range of motion and rotator cuff strength; he will then undertake tests for shoulder instability – anterior, posterior and multi-directional; it is always important to check for ligamentous laxity.
The pain x-ray will show the joint and any bony deformity at a glance. Hill sachs and Bony bankart injuries can be seen on a plain x-ray in some cases.
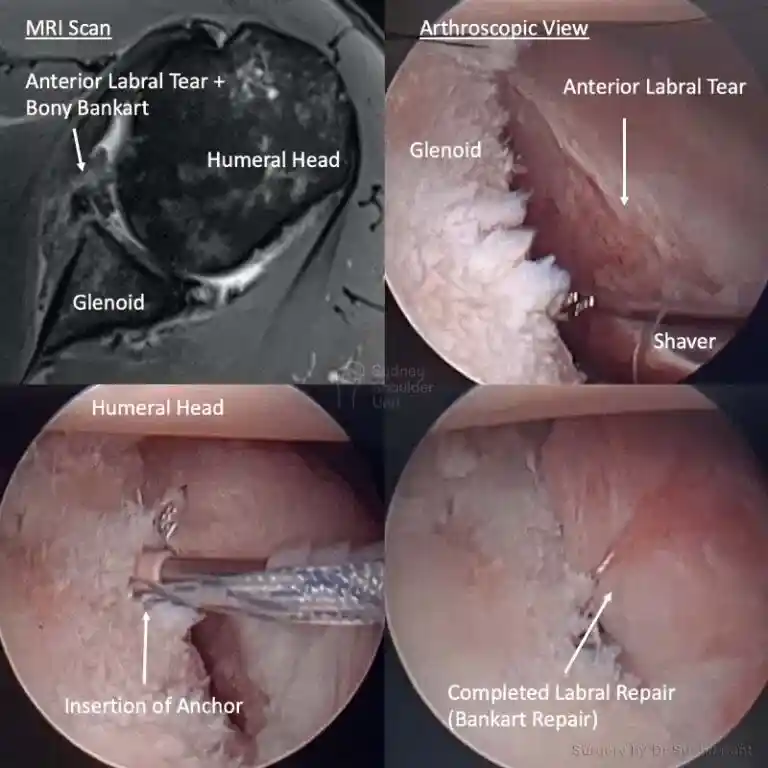
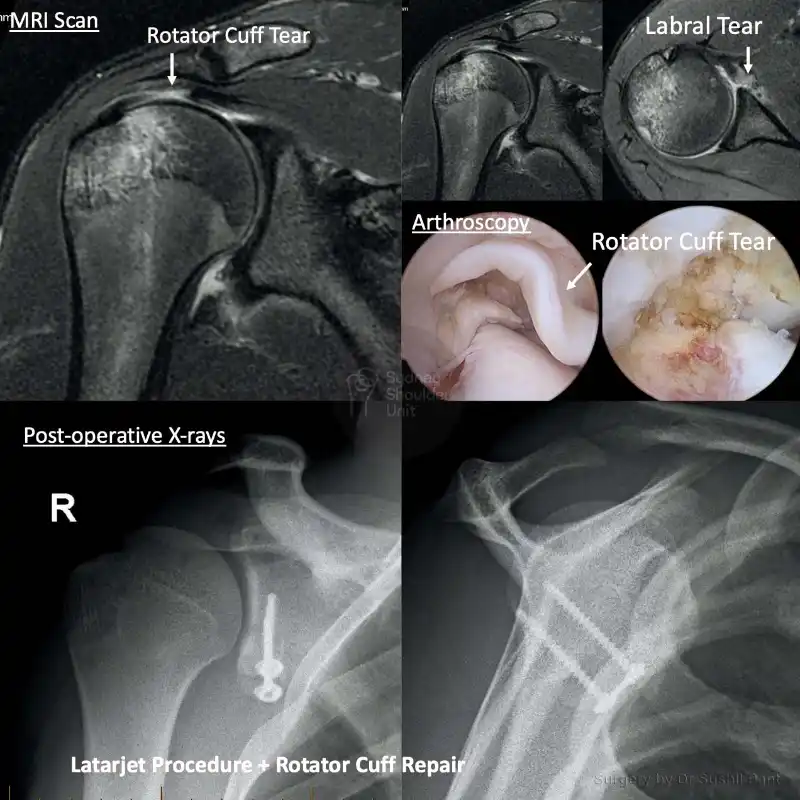
A MRI scan is almost always obtained for shoulder dislocations to look for labrum for tears (anterior and posterior), SLAP tears, rotator cuff tears, cartilage surfaces, hill sachs and bony bankart lesions. In some cases it may be necessary to obtain a CT scan with 3D reconstructions to look at any bone loss on the glenoid or humeral head in more detail.

Dr Pant utilises the JPL pathway for most patients and this will form the basis of your rehabilitation after surgery; it will be modified to suit your individual circumstance.
The JPL pathway allows for self-directed, early passive shoulder range of movement. The full JPL pathway is available for download.
Sling

When can I drive?
After shoulder surgery, you will be in a sling and you may be unable to drive for at least 6-8 weeks. This does vary depending on the complexity of your surgery and the patient. Some patients may be able to drive at 2-4 weeks, and some may not be able to drive for the full 12 weeks. This will be discussed at your follow up appointments.
Showering and getting dressed
Sleeping after Shoulder Surgery
Elbow and hand movement