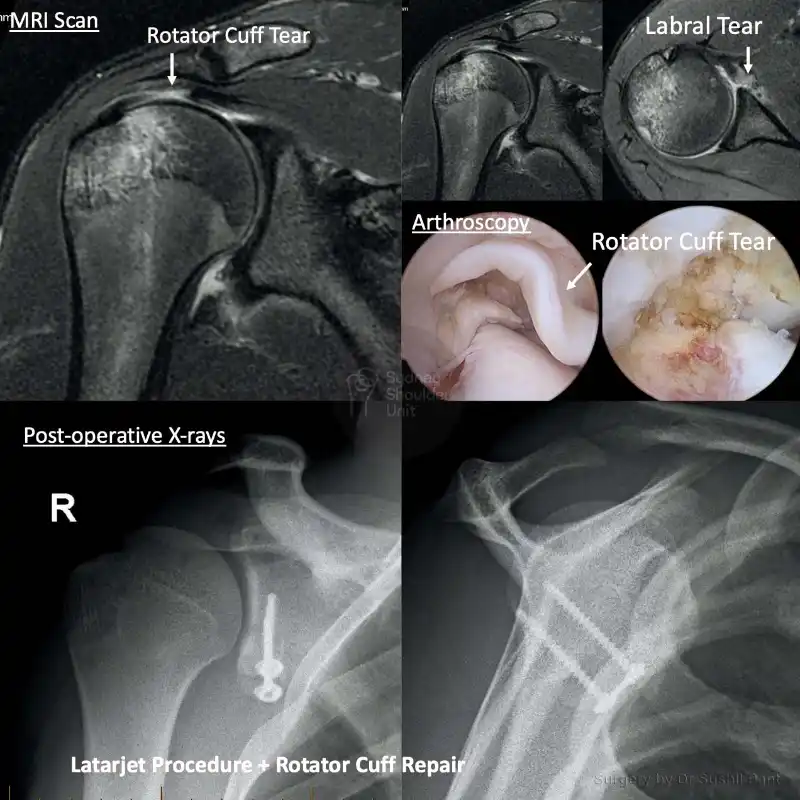
A Latarjet procedure involves transferring a piece of bone (coracoid) to the front of your glenoid (socket) to address shoulder instability (dislocations out the front). There are three reasons why this operation works so well:


Watch a surgical animation demonstrating how Dr Pant performs a Latarjet Procedure to address recurrent anterior instability in high-level athletes and overhead contact sportspersons.
https://vimeo.com/654781513
Post-operative physiotherapy
Dr Pant utilises the JPL pathway for most patients and this will form the basis of your rehabilitation after surgery; it will be modified to suit your individual circumstance.
The JPL pathway allows for self-directed, early passive shoulder range of movement:
Therapy overview
After the surgery you will be in a sling and protect your shoulder to allow the Latarjet procedure (coracoid bone graft) to heal. At two weeks after the surgery Dr Pant will see you at your review appointment and discuss the JPL rehabilitation protocol with you. This JPL physiotherapy protocol will commence two weeks after your surgery.
The therapy program will focus on flexibility and range of motion exercises initially. These gentle stretches will improve your range of motion and prevent shoulder stiffness. As the bone graft begins to heal you will be able to progress to exercises that strengthen your shoulder muscles. Shoulder strengthening is commenced at 12 weeks post Latarjet surgery.
Sling
The type of sling is selected specific to you and your shoulder surgery

When can I drive?
Showering and getting dressed
Sleeping after Shoulder Surgery
Elbow and hand movement