The Labrum is a soft tissue ring around the glenoid (socket) that deepens the shoulder joint and keeps the humeral head (ball) in the joint. After shoulder dislocations (especially recurrent episodes) the Labrum may tear off the socket and no longer function in stabilising the shoulder joint.
The labrum can tear at the:

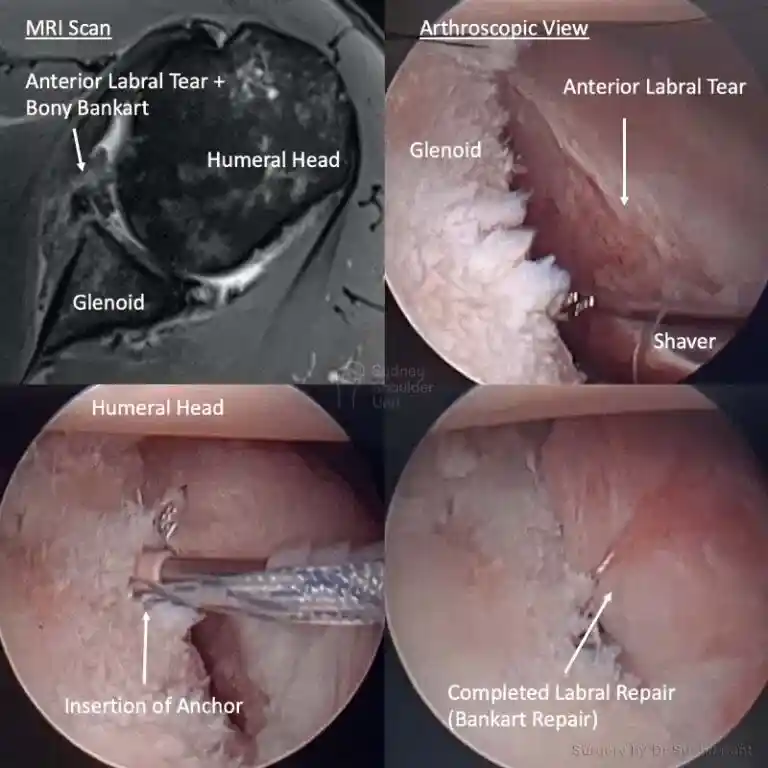
A soft tissue Bankart is essentially a “Labrum tear” as above. A bony Bankart is when the front of your socket (glenoid) fractures off or is worn out and becomes blunted over time with repeated episodes of instability. This loss of bone at the front of your shoulder will result in increased instability. The more bone you have lost at the front, the more likely it is that a Latarjet procedure is better for you. The main exception being high-level contact/overhead athletes, where the Latarjet may be a better choice from the outset (even without a bony bankart).
This is the damage (crush fracture) that occurs to the back of the ball (humerus) when it dislocates out of joint and impacts with the front of the socket. After the shoulder joint is reduced one can see a defect on the back of the ball (this is called a Hill-Sachs). The larger the Hill-Sachs lesion the more likely your shoulder is to be unstable.
Dr Pant will take a detailed history about your shoulder symptoms. He will ask about when they first began and whether there was any particular injury that caused your shoulder pain. Most patients with a Labral tear (bankart tear) recall a shoulder dislocation event which required a reduction maneuver. This may have even happened a few times with multiple trips to the emergency department. High level sports people often have an on field reduction and a period of inability to play. However, some patients may not recall a particular event. In some cases work or sport may aggravate your symptoms of shoulder instability. It is important to describe the location of pain, whether you have had any physiotherapy and injections to your shoulder.
Dr Pant will conduct a careful physical examination and check your shoulder range of motion, strength, and stability of your shoulder function. He will then perform specific tests to isolate the anterior (front) labrum, posterior (back) labrum and SLAP (top labrum) areas to see if this reproduces your symptoms of pain, apprehension and/or instability. A thorough examination is key to identifying all areas of concern around the glenoid (socket) to see how extensive your labral tear may be.
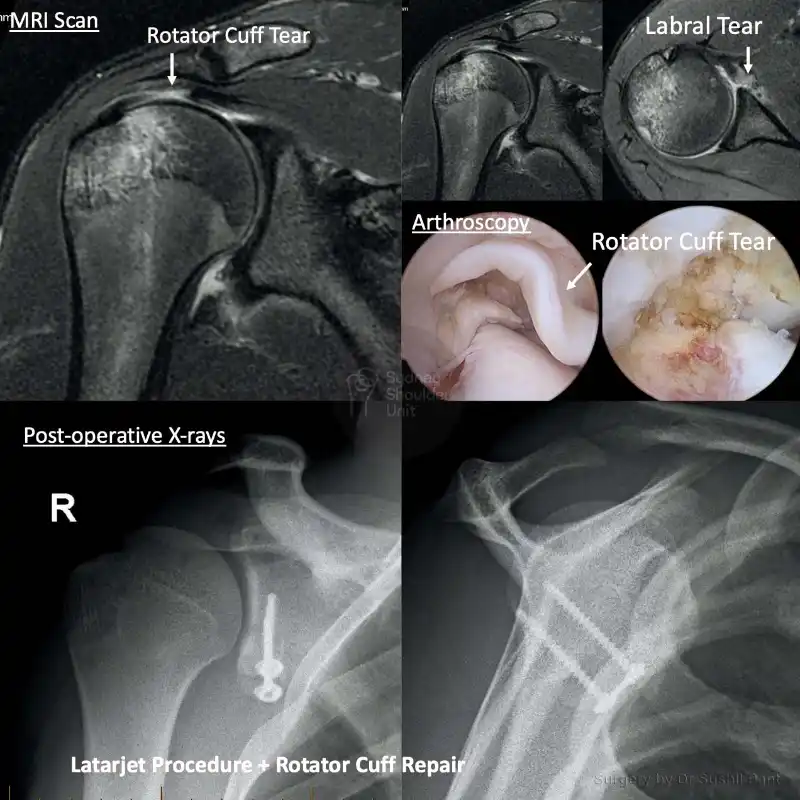
X-rays: this will show the bones of the shoulder joint in clear detail. It is a good screening test to look for any damage to the humeral head and glenoid (ball and socket). The labrum will not be seen on the plain X-ray; however, if you have a bony bankart (fracture) or a Hill Sachs on the humeral head this may be seen on a plain X-ray.

MRI scans show soft tissue better – such as the labrum. In some cases, a dye may be injected into the shoulder to help show the labrum tear (MRI arthrogram).


For most patients with a labral tear – the treatment is non-surgical. A period of rest, activity modification, and NSAIDs may be useful to treat shoulder pain.
Physiotherapy may be suggested to restore movement and strengthen your shoulder. Range of motion, rotator cuff strengthening, scapula stabilising exercise may be useful as guided by your physiotherapist. Keeping up the therapy may relieve your pain, restore your shoulder function, and prevent further injury. It may be necessary to continue this exercise program for 3-6 months in some cases.
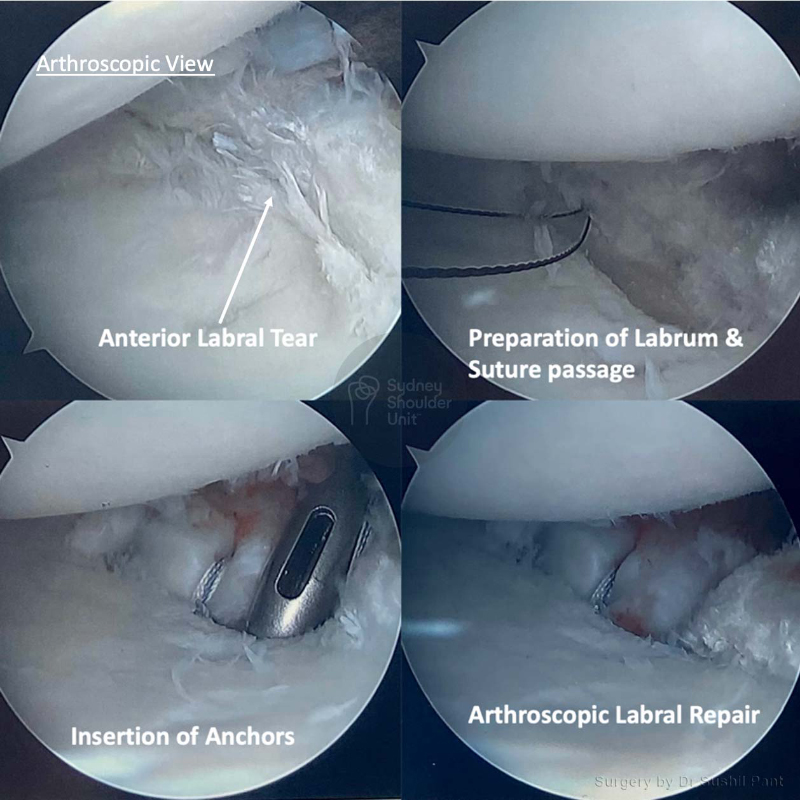
If you have not improved with non-surgical treatment or if you have a high grade labral tear (with either anterior, posterior, and/or superior extension) then you may do better with surgery. In some cases this is the best option from the outset. Dr Pant will review your case (and your CT/MRI scan) to determine if this is the right course of action to provide you with the best shoulder outcome. If surgery is required this is done keyhole (arthroscopic) and the rehabilitation is using the JPL method.
There are several different types of labral tears and Dr Pant will determine how best to treat your labral injury; in some cases, this final decision is made at the time of arthroscopic surgery. The treatment options are either “soft tissue” repair or “bone” transfer:
The factors that are considered in the treatment choices are your age, occupation, type of sport, level of sporting participation, quality of your tissue, and associated injuries in the shoulder. All of these factors need to be considered in combination to achieve the best outcome for your shoulder injury repair.
If you have glenoid bone loss (bony bankart) or you are a high-level contact athlete it may be best for you to proceed to a Latarjet from the outset. This way you only have to rehabilitate your shoulder once and you are back to full-contact sport at six months.